
Your guide to the upcoming changes
There are six key Medicare reforms that were passed in 2022 as part of the Inflation Reduction Act. Some of these changes went into effect in 2023, several more in 2024, and the final two will take effect in 2025. This article was last updated in March 2024.
Below, we outline the reforms, when they will take effect, and what people with Medicare insurance will need to know. We have also explained how PAN grants will be impacted by upcoming changes to Medicare Part D. We will update this page as new information becomes available.
Save these resources
If you or a loved one has Medicare Part D insurance, bookmark these explainers about these Medicare reforms and mark your calendar for the long-awaited financial relief. Keep reading to learn more. You can also watch our educational webinars about the Medicare reforms and upcoming changes.
- Watch our webinar: How Medicare Part D changes could lower your costs in 2024. In this webinar, we explain the changes to Medicare Part D and PAN grants in 2024.
- Watch our webinar: New Medicare reforms are law: what’s next? In this webinar, we explain the key Medicare reforms passed in 2021 and their timelines.
Changes to PAN grants
In response to the new Medicare Part D reform that will place a cap of around $3,300 on prescription out-of-pocket costs for all Medicare Part D drugs starting in 2024, we are adjusting our grant amounts beginning on January 1, 2024.
What you should know
We design our grants to cover 100% of out-of-pocket costs for most patients—and that isn’t changing. Grant amount changes will take effect when you apply for a new grant, additional funding, or to renew your grant in 2024. These new grant amounts will be available on our find a disease fund page starting January 1, 2024.
Note: Anyone issued a grant in 2023 will have access to their full, original grant amount until their grant period ends.
Additional resources
Grant amounts are changing based on disease fund, not insurance type. We’re considering all grant amounts and how what you need may change with the new Medicare reforms. If, for some reason, your PAN grant is not enough to cover your out-of-pocket costs, we offer some additional resources to help you:
- Additional funding: Patients, or their healthcare professionals, can apply for additional funding within the same initial 12-month grant eligibility period if they run out of funds and their grant balance is $0.
- FundFinder: You can use FundFinder to sign up for email or text message notifications to learn when financial assistance becomes available at any of the nine charitable patient assistance foundations.
- Referrals: We provide real-time referrals to other patient organizations if a disease fund is closed. These can be found on the individual disease fund pages.
Overview of new Medicare reforms
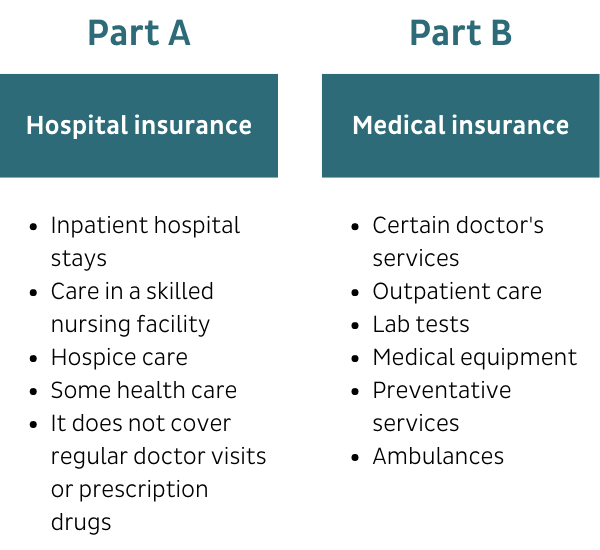
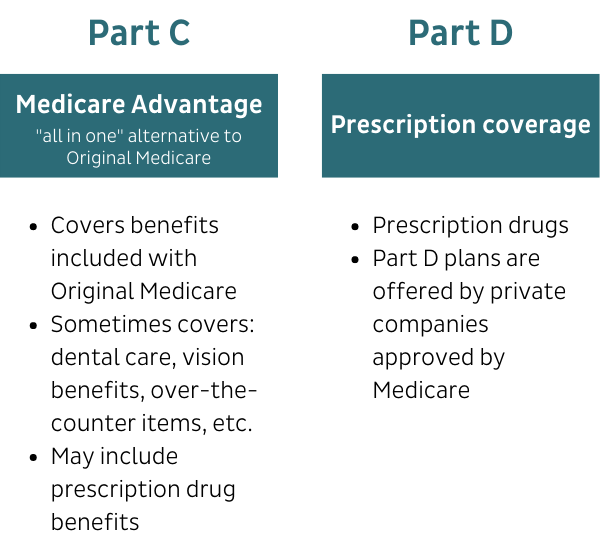
Understanding Medicare coverage
These reforms will reference different types of Medicare coverage. You may want to review what is covered by each plan before you read on:
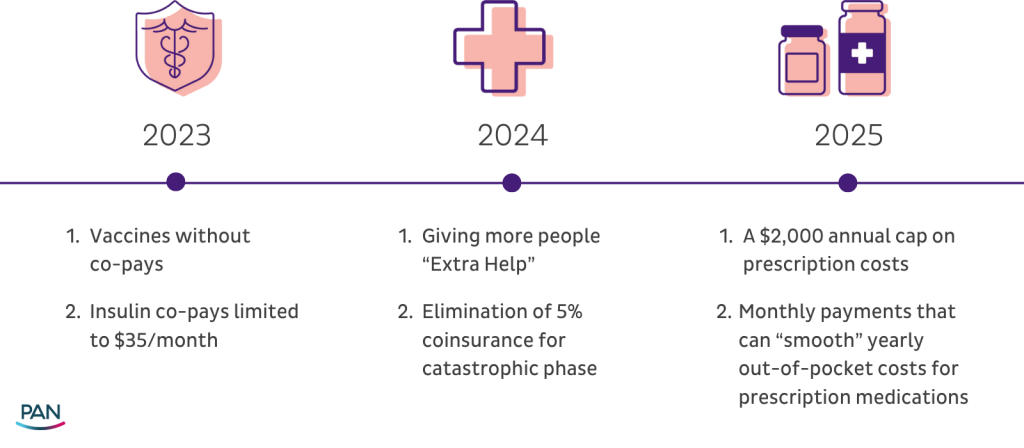
Vaccines
As of January 1, 2023, Medicare Part D plans and Medicare Advantage plans no longer require a deductible, coinsurance, or other cost-sharing requirements for adult vaccines that are recommended by the Centers for Disease Control and Prevention (CDC)’s Advisory Committee on Immunization Practices. This includes the shingles vaccine.
For a complete list of vaccines covered, see the CDC’s vaccine recommendation webpage. Vaccines currently administered in doctors’ offices and paid for by Part B do not have cost-sharing obligations.
Insulin copay monthly cap of $35
As of January 1, 2023, cost-sharing for insulin products is limited to no more than $35 per month for people with Medicare insurance, including insulin covered under both Part D and Part B. No deductibles apply. Note: plans are not required to cover all brands and types of insulin.
For a three-month supply of insulin, your costs can’t be more than $35 for each month’s supply of each covered insulin. This means you’ll generally pay no more than $105 for a three-month supply of covered insulin.
Under Part D, the $35 cap applies to everyone who takes insulin, even if you get assistance through the federal Extra Help program. If you have Part B and Medicare Supplement Insurance (Medigap) that pays your Part B coinsurance, your plan should cover the $35 per month (or less) cost for each covered insulin.
For insulin-related supplies (like syringes, needles, alcohol swabs, and gauze), you’ll pay 100 percent of the cost under Part B (unless you have Part D).
If you use a disposable insulin patch pump, you’ll continue to get your insulin through your Part D plan, and the insulin for your pump won’t cost more than $35 for a month’s supply of each covered insulin product.
- If your Part D plan covers disposable insulin patch pumps, the pump is considered an insulin supply. Because it isn’t an insulin product, the pump isn’t subject to the $35 cap and might cost more than $35.
If you use an insulin pump that’s covered under Medicare Part B’s durable medical equipment benefit, or you get your covered insulin through a Medicare Advantage Plan, your insulin costs will be capped at $35 for a one-month supply. The Part B deductible won’t apply.
- If you have Part B and Medicare Supplement Insurance (Medigap) that pays your Part B coinsurance, your Medigap plan should cover the $35 (or less) cost for insulin.
Learn more about Medicare insulin coverage.
Expansion of the federal Low-Income Subsidy (LIS) or Extra Help program
The Low-Income Subsidy (LIS) or Extra Help program is a federal program that helps people with limited income and assets pay for prescription medications and other related costs. Historically, there have been two versions of the program, the full program, which provides a higher level of financial support for people with an income of up to 135 percent of the federal poverty level, and a partial program, which provides a lower level of financial support for people with an income between 135 percent and 150 percent of the federal poverty level (FPL).
As of January 1, 2024, the partial program was eliminated. With full benefits, the majority, if not all out-of-pocket costs for prescription medications will be covered.
People who qualify for Extra Help will pay:
- No deductibles
- No premiums for Part D drug plans
- No more than $11.20 in 2024 for each brand-name drug the plan covers ($4.50 for generic medications)
- No Part D late enrollment penalty, if applicable
To qualify for Extra Help, your yearly income must be less than 150 percent of the federal poverty level and total resources must be at or below the amounts shown below. Note: these figures may each year.
2024 Yearly Income Limit*
- Single: $22,590 ($1,883 per month)
- Married (living together): $30,660 ($2,555 per month)
- *Income limits are higher in Alaska and Hawaii. If you or your spouse work, or support other family members who live with you, you may qualify for benefits even if your income is higher than the amounts shown above.
2024 Total Resource Limit**
- Single: $17,220
- Married (living together): $34,360
- **Your house, car, and up to $1,500 per person in burial expenses don’t count as resources.
Some people get Part D Extra Help automatically. If you fall into one of the categories below, you do not need to apply for Extra Help:
- You’re enrolled in both Medicaid and Medicare (“dual eligible”).
- You receive Supplemental Security Income (SSI).
- You qualify for a Medicare Savings Program.
To learn more and check your eligibility:
- Medicare.gov has a resource to help you quickly see if you qualify for Extra Help.
- You can enroll in the Extra Help program by visiting SSA online at ssa.gov/ExtraHelp or call 1-800-772-1213. Visit ssa.gov/locator to get the telephone number for your local Social Security office.
- For one-on-one assistance with Extra Help, contact your State Health Insurance Assistance Program (SHIP) at ShipHelp.org or call 1-877-839-2675 to get the number for your local SHIP.
- You can also visit PAN’s Extra Help education hub to learn more about this program and see if you qualify.
Elimination of the five percent coinsurance for Part D catastrophic coverage
As of January 1, 2024, people with Medicare Part D are no longer responsible for five percent prescription cost-sharing in the ‘catastrophic phase’ of coverage. This means that once a person reaches the catastrophic phase of coverage in 2024, they have no out-of-pocket responsibility for covered drugs for the remainder of the year.
With this change in effect, Part D enrollees who take only brand-name drugs in 2024 will have a cap of about $3,300 for calendar year 2024, according to a February 2024 Kaiser Family Foundation brief.
However, the Centers for Medicare and Medicaid (CMS) estimates that for some people enrolled in Medicare Part D who have very high drug costs, their out-of-pocket costs will be capped between $3,300 to $3,800
This change will have the biggest impact on people with Part D who have expensive medications, and who don’t qualify for the Extra Help program. They could save thousands of dollars on their covered medications.
Annual limit of $2,000 for prescription drug costs in Part D
Beginning in 2025, people with Medicare Part D will have an annual limit, capping their out-of-pocket prescription drug costs at $2,000. In the years that follow, annual limits will be adjusted based on inflation. This cap does not apply to out-of-pocket spending on Part B drugs. Medicare Part B covers drugs that are administered by a doctor, nurse, or other healthcare provider in an outpatient setting such as a doctor’s office. For example, some cancer drugs and injectable drugs are covered under Part B.
Read more about the Part D cap below.
This will have the biggest impact on people with Part D who have expensive medications and who don’t qualify for the Extra Help program.
For example, someone who usually has drug costs high enough to reach the catastrophic threshold could save about $1,300 in 2025, compared to their 2024 spending.
Option to smooth out-of-pocket prescription drug costs in monthly installments
Beginning January 1, 2025, each Medicare prescription drug plan, including Medicare Advantage plans with drug prescription programs, must give patients the option to pay for their out-of-pocket prescription costs in monthly installments, with a monthly limit on spending. At PAN, we have called this provision smoothing, as it more evenly distributes costs throughout the year.
Please note that patients will need to enroll in smoothing. Monthly payment plans will not be automatic.
Read more about part D smoothing below.
Cost and coverage impacts
Changes to insurance coverage
These changes will not affect an individual’s current Medicare enrollment and should not impact decisions during open enrollment. During open enrollment, we encourage people to select plans that best match their current prescription and medical needs.
The Medicare reforms apply to all Part D plans and Medicare Part C or Medicare Advantage plans that have prescription drug coverage. Medicare HMO plans are included if they offer drug coverage. The reforms do not apply to supplemental insurance or Medigap plans, or Red, White & Blue insurance, which covers Parts A and B of the Medicare program.
| Medicare reforms apply to | Medicare reforms DO NOT apply to |
| All Part D plans | Supplemental insurance |
| Medicare Part C—or Medicare Advantage—plans with prescription coverage | Medigap plans |
| Medicare HMO plans, if they offer prescription coverage | Red, White, and Blue insurance |
These reforms should not impact your medication choices
Medicare reforms, such as the Part D cap and smoothing, apply to all medications covered by the Medicare program, including those on specialty tiers. No drugs are excluded. You will not have to change medications in order to benefit from the Part D cap and smoothing. The Medicare reforms will apply if you are taking a brand or generic medication.
What medication is best for you is a decision between you and your healthcare provider. During the open enrollment period, we recommend that you pay close attention to any changes in your current plan related to medications you may need, and carefully review a potential new plan’s drug coverage and related copays and coinsurance.
Out-of-pocket prescription drug costs after the new reforms
In 2024, after paying the initial deductible, a person on Medicare will pay 25 percent of drug costs. They will have a cap of about $3,300 and will no longer pay five percent of drug costs in the catastrophic phase.
In 2025, after paying the initial deductible, a person on Medicare will pay 25 percent of drug costs. They will not spend more than $2,000 a year in out-of-pocket costs for their prescription medications. (The annual cap amount will be adjusted based on inflation in the years that follow.)
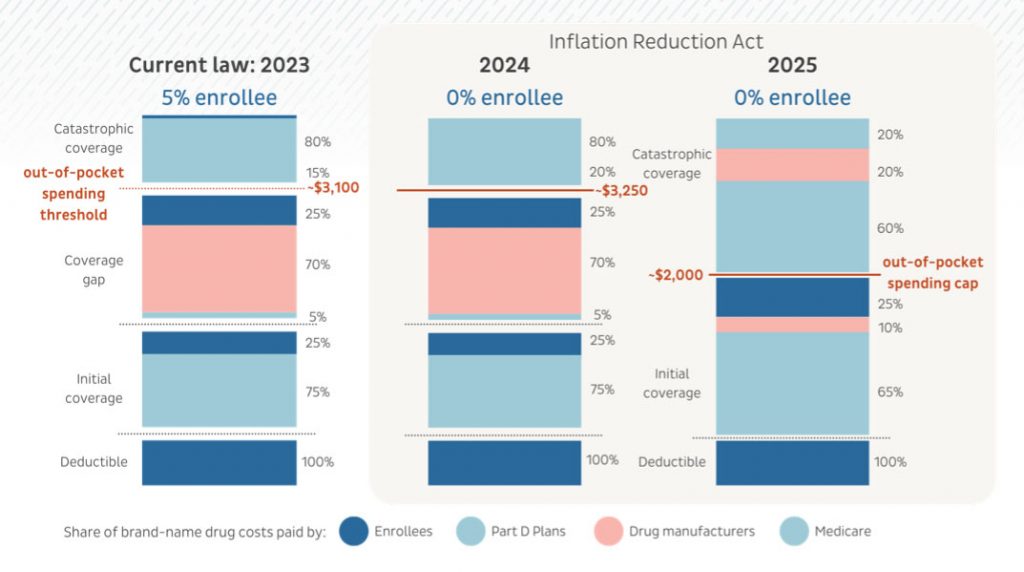
Cost-sharing in the catastrophic phase has been decreased for 2024 and will be eliminated in 2025. Patients will continue to pay copays at the pharmacy counter until they reach the Part D cap of $2,000 in 2025.
Changes to Medicare Part D premiums
The Inflation Reduction Act included a provision that prevents “Medicare Part D base beneficiary premiums” from increasing more than six percent each year. Unfortunately, the base beneficiary premium is not the same as the amount that Part D enrollees pay for coverage, and the law did not cap the growth in individual plan premiums to six percent. Health plans use the base beneficiary premium to calculate their plan’s basic premiums, but they also consider other factors.
This IRA premium provision is effective from 2024 to 2029, so the base beneficiary premium is limited to six percent increases each year, but plans are not limited in other increases.
Patients should carefully review their plans during open enrollment to ensure they are considering all out-of-pocket costs and coverage.
Using discount cards and drug manufacturers’ assistance
By law, drug manufacturer patient assistance programs cannot assist people with federal insurance, including Medicare. Drug manufacturer assistance programs support people who are uninsured and people with commercial insurance. For example, manufacturer coupon cards may be available for those with commercial insurance seeking access to particular branded medications.
About the Part D cap
The $2,000 cap does not apply to prescriptions under Part B
The $2,000 cap only applies to Medicare Part D plans and Medicare Advantage programs with prescription drug plans and does not apply to drugs covered under Medicare Part B.
The cap only applies to covered medications
The Part D cap only applies to medications that are covered by a patient’s Medicare prescription drug plan. Part D plans may choose to not cover certain drugs. However, they are required to cover medications that fall into one of the six protected classes: immunosuppressant (organ transplant), antiretroviral (HIV/AIDS), antidepressant, antipsychotic, anticonvulsant (seizures), and antineoplastic (cancer). Drug plans must cover at least two drugs in other categories.
If you are prescribed a drug that is not covered by your prescription drug plan, here are some options:
- If the non-covered prescription drug is a brand-name medication, ask your doctor whether a generic equivalent might work (if there is one).
- Find out whether there are any other prescription drugs in your plan’s formulary that would be effective.
- Your physician can try a formulary exception, a request to obtain a Part D drug that is not included on a plan’s formulary. If the plan denies the request, there is an appeals process.
- During the Open Enrollment Period, October 15-December 7, evaluate the plans available to you. You might find one that covers your needed medication.
Please note, if you choose to pay for a medication that is not covered by your prescription drug plan, your payment will not apply toward the Part D cap of $2,000.
Tracking payments toward the cap
The patient’s Part D plan or Medicare Advantage drug plan will be tracking costs and will determine when the cap has been met.
Income requirements for the Part D cap
Anyone with a Medicare Part D plan or who is enrolled in a Medicare Advantage program with a prescription drug plan will automatically have a Medicare Part D cap in 2025. There are no eligibility requirements, including income.
About Part D smoothing
A new name for smoothing
The Centers for Medicare & Medicaid Service (CMS) are using a new name to describe “smoothing.” It will now be the Medicare Prescription Payment Plan.
Medicare Prescription Payment Plan timeline
Beginning in 2025, anyone with a Medicare Part D prescription drug plan will have the option to enroll in the monthly payment plan, either before the beginning of the plan year or in any month during the plan year. The opportunity to enroll is not income-based.
The Medicare Prescription Payment Plan only applies to out-of-pocket costs for prescription medications. Payments will not include premiums.
Monthly payments under the Medicare Prescription Payment Plan
While CMS has not finalized how the Medicare Prescription Payment Plan will operate in 2025, preliminary guidance suggests the following:
- The Medicare Prescription Payment Plan is completely voluntary; patients will need to “opt-in” to the program.
- Participants will not have any monthly bills until they opt into the program AND have out-of-pocket prescription costs.
- Once a participant has out-of-pocket prescription costs, they will be billed on a monthly basis. This will continue as long as they remain part of the Medicare Prescription Payment Plan.
- All out-of-pocket costs will be billed monthly, including costs during the initial deductible phase. In other words, participants will not need to spend a certain amount out-of-pocket before they can join the program.
In 2025, people with Medicare Part D will have a $2,000 annual cap on out-of-pocket costs, but determining what a participant in the monthly plan owes each month is not as simple as $2,000 divided by 12 months.
Monthly bills will be calculated by starting with the annual out-of-pocket maximum, which in 2025 will be $2,000. First, the plan will subtract any Part D costs the participant paid out of pocket before joining the monthly program. Then, the plan will divide the remaining costs across the remaining months in the plan year. CMS will be developing monthly calculators to help patients know what their monthly costs will look like, and to determine if enrolling in the Medicare Prescription Payment Plan makes sense for them.
Consider the following example:
A woman named Ruth is interested in the Medicare Prescription Payment Plan, and she enrolls in January 2025. She has no out-of-pocket costs in January, but she fills her first prescription in February. Her out-of-pocket responsibility is $1,030.37.
- Step one: Determine Ruth’s total annual out-of-pocket maximum, which is $2,000 in 2025.
- Step two: Subtract Ruth’s out-of-pocket costs before she joined the Medicare Prescription Payment Plan. She had none, so this total is $0.
- Step three: Calculate Ruth’s monthly payments, by dividing her total costs across the remaining months in the plan year. Ruth filled her prescription in February, so she will divide her payments over 11 months. Her out-of-pocket prescription cost is $1,030.37, so that amount will be divided across 11 months. Her monthly bill will be $93.67.
If Ruth later had additional out-of-pocket prescription costs, her monthly bill would have to be recalculated. Her annual total will not exceed $2,000, but her monthly payment could change.
Remember, the annual cap will begin at the same time as the Medicare Prescription Payment Plan, so the maximum amount a person with Medicare Part D will pay is $2,000 per year.
| Month | OOP Costs Incurred | Maximum Monthly Cap | Monthly Participant Payment |
| January | $0 | $166.67 | $0 |
| February | $1,030.37 | $93.67 | $93.67 |
| March | $0 | $93.67 | $93.67 |
| April | $0 | $93.67 | $93.67 |
| May | $0 | $93.67 | $93.67 |
| June | $0 | $93.67 | $93.67 |
| July | $0 | $93.67 | $93.67 |
| August | $0 | $93.67 | $93.67 |
| September | $0 | $93.67 | $93.67 |
| October | $0 | $93.67 | $93.67 |
| November | $0 | $93.67 | $93.67 |
| December | $0 | $93.67 | $93.67 |
| Total | $1,030.37 | $1,030.37 |
The guidance for how the Medicare Prescription Payment Plan will be operated is not yet final, but we will share updates when the plan is finalized.
More reforms are needed
Dental, vision, and hearing benefits for people on Medicare
At PAN, we have long advocated for the expansion of dental, hearing, and vision benefits in the Medicare program. Unfortunately, the Inflation Reduction Act did not expand these benefits.
However, the U.S. Food and Drug Administration (FDA) established a new category of over-the-counter hearing aids in 2022, allowing people to buy over-the-counter hearing aids in stores and online, without needing a hearing exam, prescription, or fitting appointment.
Prior authorization likely to change
While the Inflation Reduction Act did not include changes relating to restrictive utilization management practices, the Centers for Medicare and Medicaid Services has issued rules to improve the process of prior authorization. Once the rules become final, Medicare Advantage plans, fee-for-service and managed care Medicaid and CHIP programs, and Affordable Care Act marketplace plans will be required to streamline the prior authorization process.
The rules require these payers to implement an electronic prior authorization process, shorten decision times for payers to respond to prior authorization requests, and require payers to provide a specific reason for denying a prior authorization request. The rules also include other provisions to boost transparency around the prior authorization process and promote health data sharing overall. The timeline for finalizing the rules is unknown.
Impacts on people without Medicare
In 2021, the American Rescue Plan Act temporarily lowered healthcare costs for most Marketplace consumers by increasing financial assistance based on income level. These short-term subsidies were set to expire at the end of 2022, but the Inflation Reduction Act included a provision that extends these enhanced premium subsidies through the end of 2025.
Additional resources
Stay updated about Medicare reforms
Medicare and your Part D plans should share information about the Medicare reforms before they go into effect. PAN will continue to educate patients and providers about important timelines and next steps. The latest information will be included here on our Medicare reforms webpage.
Learn more with these key resources
- Visit Medicare.gov or call 1-800-MEDICARE (1-800-633-4227).
- Visit the National Council on Aging for resources and information about Medicare.
- Contact your local State Health Insurance Assistance Program to receive free, personalized health insurance counseling.
- You can enroll in the Extra Help program through the Social Security Administration online at ssa.gov/ExtraHelp or by phone at 1-800-772-1213.